
Two Predisposing Causes of Back Pain Everyone Needs to Know About
This is probably the most important article I have written to date. I know most of you won’t read it because of its length. If you do read it, you will know more about the cause and prevention of back pain than most health professionals who treat this problem. If you or someone close to you has ever had their back “go out” or developed a chronic, recurring backache, this article explains why. I will also share with you the best thing you can start doing right now that has helped me and thousands of my patients overcome back pain.
I have been treating spine problems for over 20 years and I have observed that back pain presents itself in one of three scenarios…
Scenario 1: You are getting yourself ready to go about your day, you bend forward to put on your socks or pick something up and all of a sudden your back “goes out” and you feel a sharp, stabbing pain. You have difficulty understanding how this could possibly happen. It wasn’t anything strenuous. “All I did was bend over!”
Scenario 2: You bend forward to lift something heavy and when you go to lift, again your back “goes out” and you feel a sharp, stabbing pain. This one you can understand. It was fairly strenuous. “Maybe I lifted the wrong way?”
Scenario 3: The muscles in your back begin to tighten up and you develop a deep dull ache. It may have been from some activity you did from the previous day or it started for no apparent reason. There was no immediate “incident” that set it off. It does get better, but always seems to come back from time to time.
I discuss more on why these scenarios happen later in the article.
If any of you have been lucky enough to experience all three scenarios like I have, you know how bad back pain can be, especially when it is so difficult and painful to get out of a chair, lift a leg up, or turn over in bed. There comes a time when your back becomes such a nuisance you need professional help.
You likely go one of two routes…
The Medical Route
You have a not so thorough exam, an x-ray or maybe an MRI and they don’t see any problems…no fracture, no bulging or herniated disc, no spinal degeneration (arthritis). They are unable to explain why you are in pain when they don’t see any problems on your x-ray or MRI.

MRI demonstrating bulging and herniated discs
Or they do see a bulging, herniated, or degenerated disc and this is what they tell you. They are unable to explain why you have this “damage” in your spine. They commonly tell patients that the problem is due to “aging” or “normal wear and tear.” These are the lamest reasons I have ever heard since my time working in this field. Most patients buy into this line of thinking because it makes intuitive sense, but in reality it doesn’t. If this was true, we would find that EVERYONE has an equal amount of disc and joint wear in EVERY JOINT IN THEIR BODY AS THEY GET OLDER. We simply DO NOT SEE THIS! What we do see is wear and tear in selective joints in selective people. It is occurs in the joints that are least stable and have the worst movement mechanics, not aging and “normal” wear and tear.
The bottom line is signs of spinal degeneration and disc pathologies indicate a long-term “wear and tear” process…not a good thing. Spinal pathologies are mostly what conventional medical professionals are screening for and they aren’t too concerned about the predisposing causes I am going to talk about. In either case, they may recommend a course of anti-inflammatory drugs, a cortisone injection, surgery, or they send you off to physical therapy.
Or you decide to go the…
The Chiropractic Route
You have a bit more thorough exam and you may or may not have an x-ray, depending on the chiropractor’s philosophy and approach. The chiropractor may rub your back, put you on therapy machines and then “cracks” your spine in a few places. Not to say these don’t have some short-term, pain relieving benefits, but these do nothing to address the predisposing causes I am about to talk about.
The 3 Questions Most Spine Specialists DON’T Ask Themselves
Most medical professionals, physical therapists, and even chiropractors don’t ask themselves these questions about the patients they are treating:
- “Why did this patient develop a “damaged” disc?”
- “What is wrong with this patient’s posture and movement habits that has caused this to happen?”
- “What is the best treatment, exercises and movement habits I can teach this patient for the best recovery AND reduce the chances of this happening again?”
If these “specialists” do not ask themselves these questions, it will be very difficult for them to find the long-term solutions to their patient’s problems. Been there, done that! These are the questions that burn in my brain every day!
The Two Predisposing Causes of Back Pain
There are two predisposing causes of back pain that most people don’t know about, including many health professionals that treat back pain! The first one has to do with…
Alignment
When I am talking about alignment, I am referring to the alignment of the spinal column and posture. I am also referring to both “static” alignment, such as when sitting or standing still, as well as “dynamic”’ alignment, when our body is in motion.
Ideal alignment of our spine and body as a whole (posture) is vital for not only the long term health of our musculoskeletal system, but it is also a factor for our overall health as well.
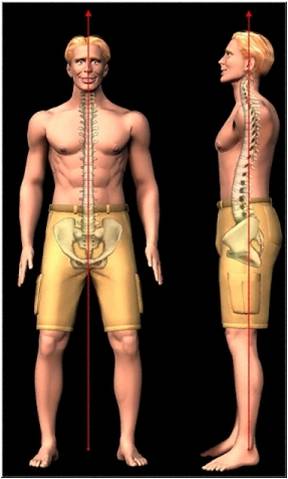
Ideal Static Alignment of the Spine and Posture
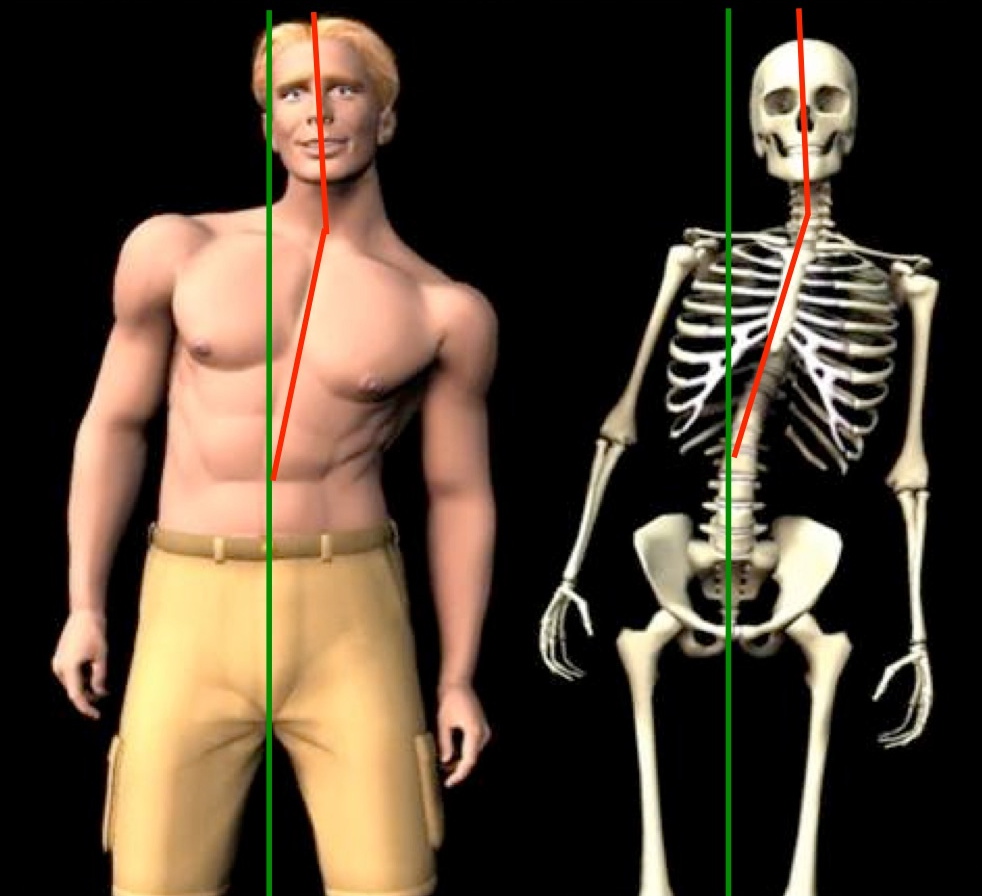
Abnormal Static Alignment of the Spine and Posture
Many of us lose proper “static” alignment of our spine and posture due to the injuries we acquire throughout life. Sudden, traumatic injuries, such as a fall, sports injury, or car accident often cause the spine to shift out of place. Working, sitting, or sleeping in a bad posture for extended periods of time can do the same.
Many of us lose proper “dynamic” alignment because we have simply lost the ability to move correctly. We all learned to move and move flawlessly in our first few years of life when we went through the developmental milestones. After years of injuries, compensating for those injuries, and the impact a more sedentary, industrialized lifestyle has had on our bodies, we have paid the price by developing poor movement habits. The best example of this is when people lose the ability to move in their hip joints when they bend, squat, or twist their body. They compensate by bending and twisting more in their lower back. What happens over the long haul? You guessed it, back pain. Many people are in pain because they simply don’t move right!

Shoulder joint demonstrating proper dynamic alignment (centrated joint) when the arm is lifted overhead.
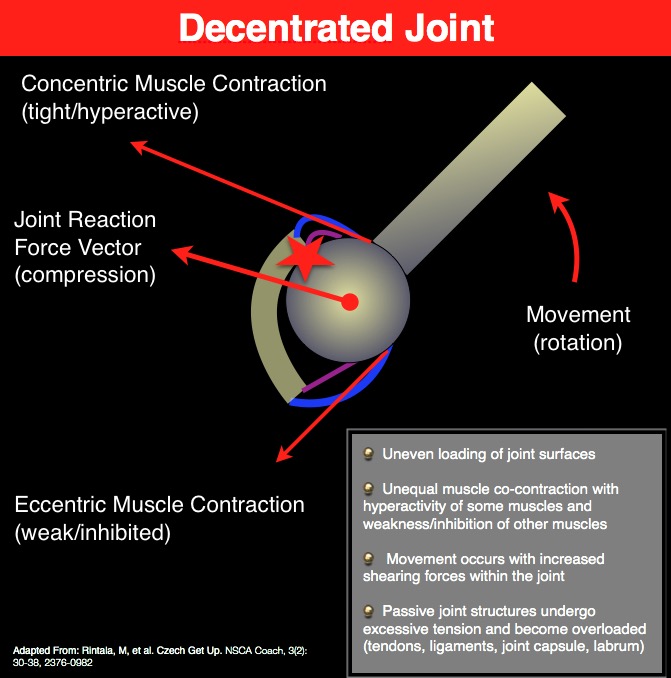
Shoulder joint demonstrating poor dynamic alignment (decentrated joint) when the arm is lifted overhead.
If we lose proper alignment statically or dynamically, there will be excessive loads (compression, tension, torsion, shear) on spinal tissues weakening them over time. This leads to scenario 1, 2, or 3.
The second predisposing cause of back pain has to do with…
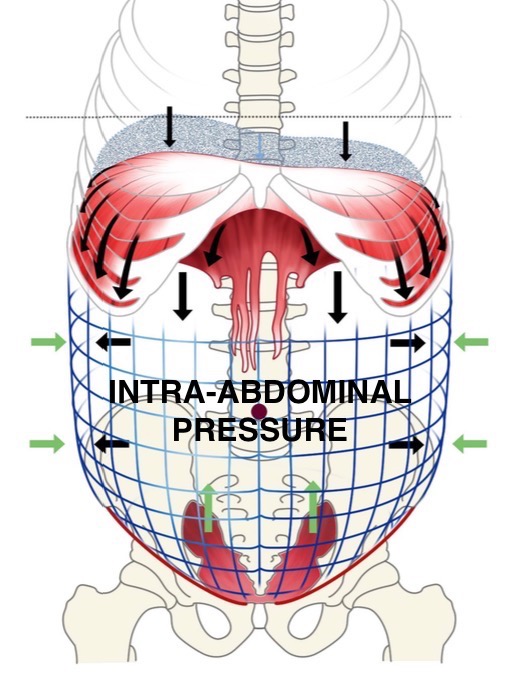
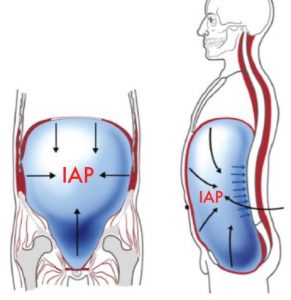
Intra-Abdominal Pressure (IAP)
IAP is the mechanism that stabilizes our spine. It is essentially our “built in” back brace. This is the most important new discovery in the last decade and it is a game-changer for the difficult patients with back pain who don’t get completely better with chiropractic treatment, physical therapy, or their back pain always comes back from time to time.
IAP should be an automatic, subconscious activation of your core before and during every movement you make. The problem is, the vast majority of people who suffer with back problems have lost this automatic ability to create IAP when they bend and move. When IAP is insufficient, spinal tissues begin to pay the price.
Two Common Reasons Why People Lose The Ability to Create IAP
Pain, Trauma, and Injuries. Our bodies have unique ways of creating compensations for physical and emotional trauma. Unfortunately, one of them is an alteration in how we stabilize our core. The automatic ability of creating IAP becomes absent, delayed, or lost during movement.

Poor Core Stabilization Strategy
Pulling the abdomen in and lifting the chest does not increase IAP and makes the spine unstable.
Cosmetic, Cultural or Learned Behavior. Some people “suck in” their stomach in an attempt to look thinner. Other people are taught to “suck in” or “pull in” their stomach as an exercise to activate their core. Even though some abdominal muscles are contracting when they pull their belly button towards their spine, they are contracting their muscles in the exact opposite direction that is needed to create IAP and increase spine stability. If this “pulling in” strategy becomes habit, it will have a destabilizing effect on the spine which will eventually lead to pain and wear and tear on spinal tissues.
How Problems With Alignment and IAP Lead to Back Pain:
The 3 Scenarios
Problems with alignment and IAP create the perfect storm for the eventual development of back pain and the often associated “wear and tear” spinal pathologies (disc annular tears, bulging, herniations, protrusions, degeneration, arthritis, stenosis, ligament hypertrophy, etc.)
Alignment problems will predispose people to back pain because spinal tissues will be pre-stressed most of the time. Poor static alignment will expose certain discs, muscles, ligaments, nerves, etc. to higher loads compared to ideal alignment. Tissues under greater stress and strain will be more prone to injury, wear and tear and pain generation over time. The bottom line is poor static alignment will increase the likelihood of developing back pain in any of the three scenarios mentioned at the beginning of this article.
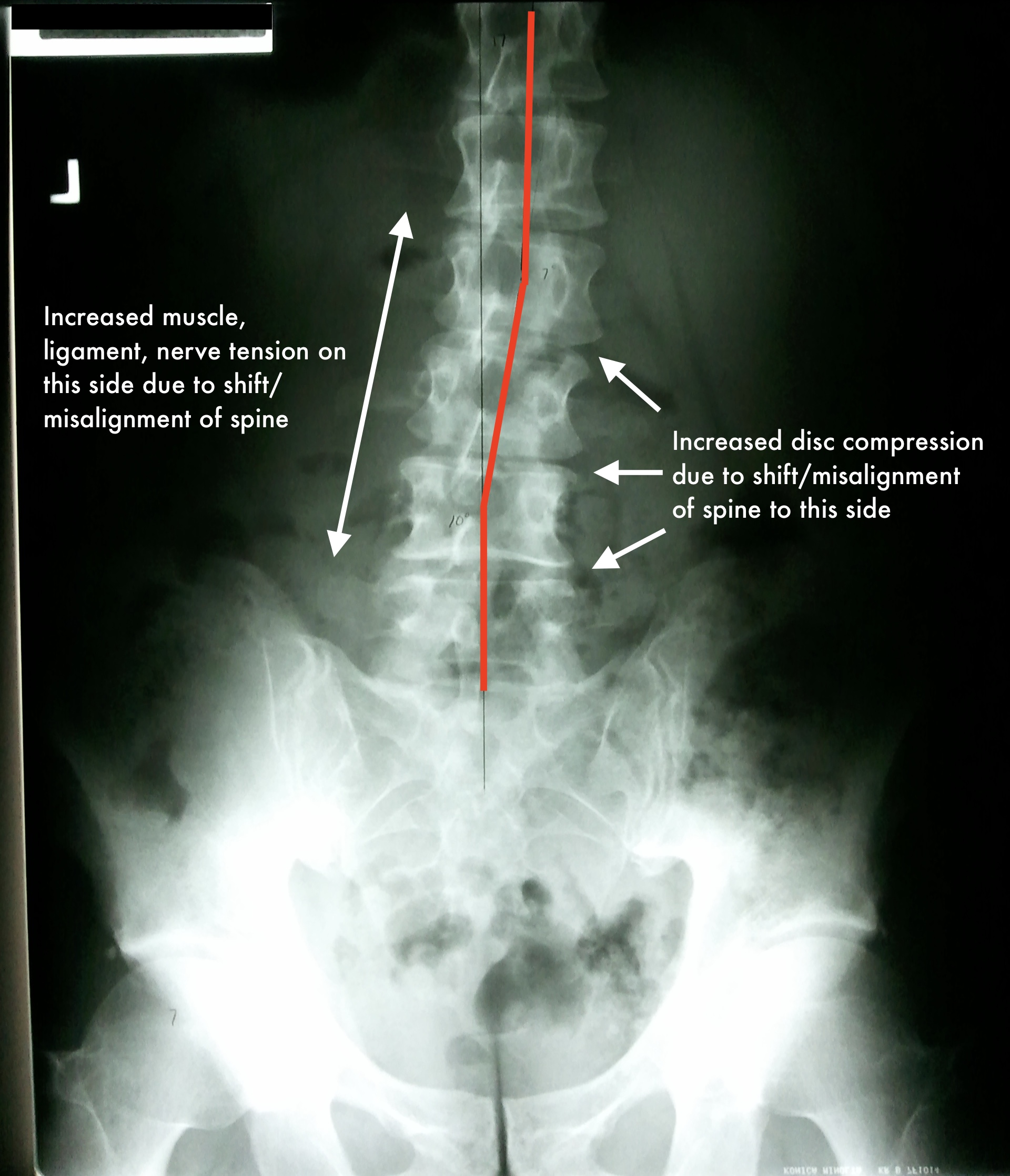
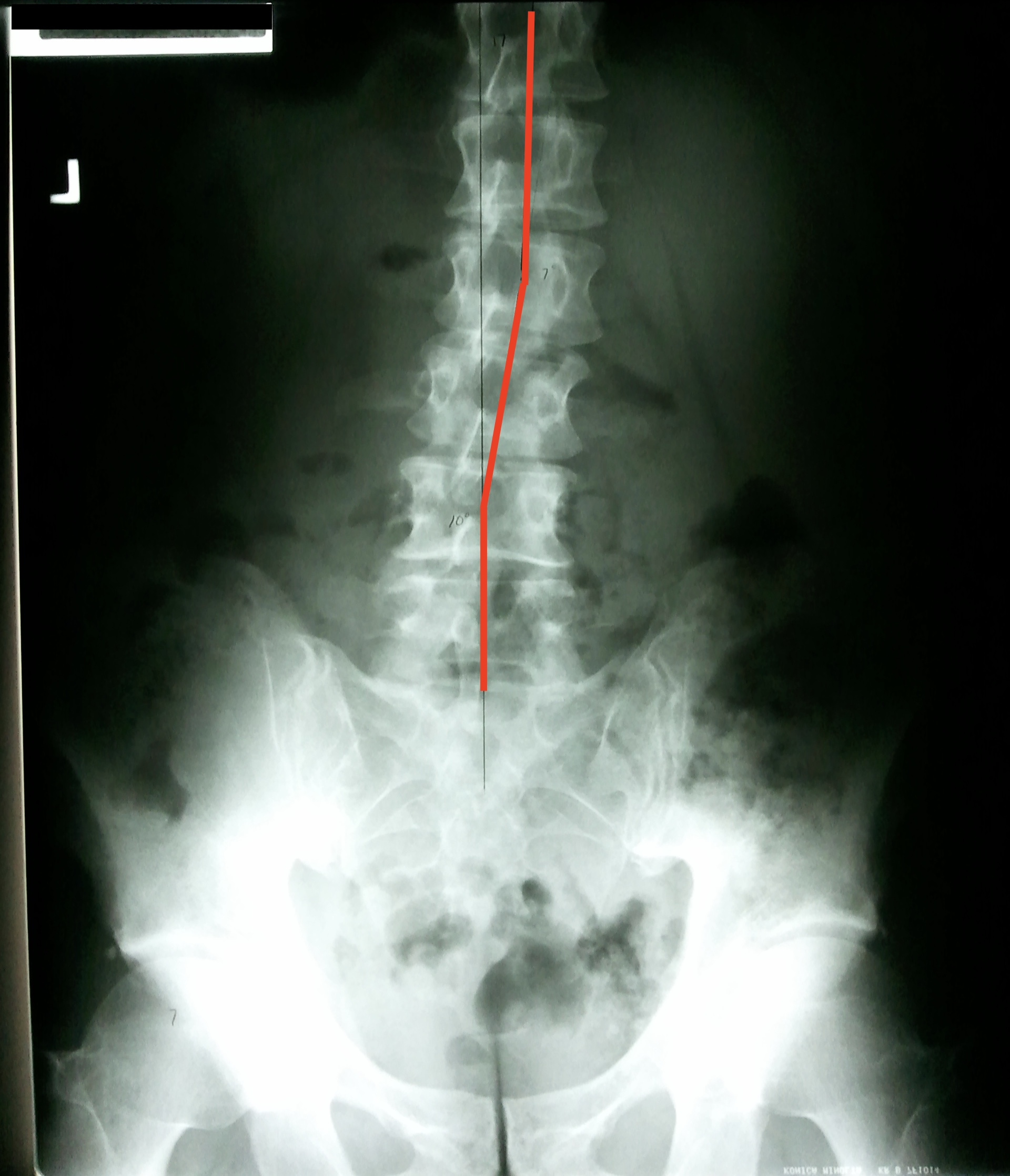
X-ray of a misaligned spine in one of my patients with multiple herniated discs and sciatica (leg pain)
IAP problems will predispose people to back pain because the spine is not stabilized properly during movement. Another way of saying it is, IAP takes stress off the spine. If you do not create and maintain IAP during movement, more stress is transferred to spinal tissues. This ends up creating thousands of micro “insults” (small injuries) to the spine every time you move, bend, lift, etc. You don’t feel them until your spinal tissues have become so weak and damaged to the extent that it only takes one more bend of your back to set it off…The straw that broke the human’s back! This is exactly what happens in Scenarios 1 and 2.

The Lumbar Extension Stabilization Strategy
Scenario 3 is like 1 and 2 in that it is usually a combination of an alignment and an IAP problem. Poor alignment stresses spinal tissues over time and eventually you feel tight muscles in your back or a deep, dull ache in your joints or discs. Lack of IAP also stresses spinal tissues. If you can’t create adequate IAP, you have an option to compensate for this by adopting a lumbar extension stabilization strategy. That is, you tighten up your lower back muscles causing it to arch too much to create some semblance of core and spine stability. Unfortunately, this is not an effective long-term solution to the IAP problem. If this strategy persists for too long, back muscles become chronically tight, overused and painful, spinal discs become injured because they are highly compressed, and low back pain eventually develops. This is an epidemic problem I see every day!
Alignment and Intra-abdominal Pressure:
The Keys to a Healthy Back
Now that you know alignment and IAP are the two predisposing causes of back pain, what can you do to fix these problems?
How to Fix Your Alignment
When the spine shifts out of place and becomes misaligned, it usually can’t go back into place on its own. This is where chiropractic comes in. And not just any chiropractor. It needs to be a “corrective” chiropractor. There are many types of chiropractors with varying philosophies and approaches. Corrective chiropractors are trained in the best methods to correct the alignment of the spine. There are several different corrective chiropractic techniques, but the one that stands above all others is Chiropractic Biophysics Technique (CBP). It is the most effective, scientific and researched method of all chiropractic techniques with over 200 studies validating its approach. For these reasons, I highly recommend a chiropractor trained and certified in CBP technique.
X-ray of one of my patients BEFORE CBP corrective care. He had multiple herniated discs, back pain, sciatica, and a failed back surgery
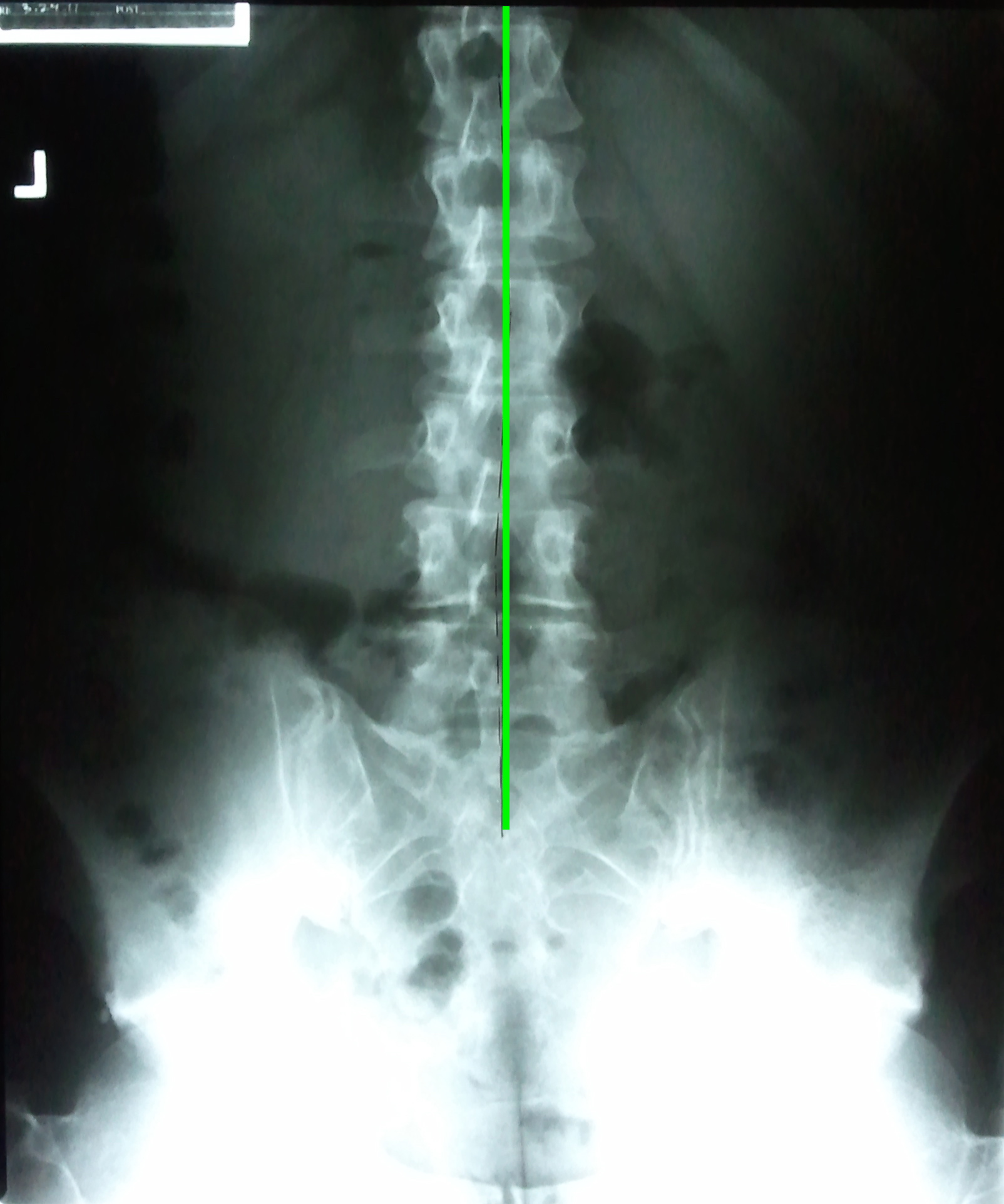
X-ray AFTER a program of CBP corrective care. Back pain and sciatica resolved
Find a CBP chiropractor near you
So if your spine is out of place and misaligned (x-rays and posture assessment will verify this), there is not much you can do about this on your own without the help of a corrective chiropractor. They need to determine from your x-rays and posture what spinal adjustments, exercises, or other treatment you might need to correct your spinal alignment to as near normal as possible.
How to Fix IAP
What you can work on and usually improve on your own (if you do it and implement it correctly) is your ability to create IAP when you bend, move, lift, etc.
Place your hands around your waist and cough or make a hard “CHA” sound. You should be able to feel how your abdominal muscles tighten up and pressure builds inside your abdomen. This is IAP! Two things have to happen to create good IAP. The diaphragm, which most people know as the primary breathing muscle, contracts and pushes down into the abdomen and at the same time the abdominal and pelvic floor muscles tighten up. This builds up pressure inside the abdomen which stabilizes and keeps the spine from bending when it shouldn’t bend. It also stabilizes the spine when the spine does need to bend. In both instances, it is this pressure that protects the spine from injury.

How to Assess Your Ability to Create IAP
Place your hands around your waist. Suspend your breath (no breathing), push out into your hands, and tighten up/flex your abdominal muscles at the same time. Think about tightening up your abdominals as if someone is going to punch you in the stomach. If you do it correctly, you should feel pressure build inside your abdomen (IAP) and all parts of your abdominal wall move outward and tighten up. If you are unsure, cough a few times and that is the feel you are looking for. You should feel symmetrical outward excursion and tightening of your entire abdominal wall, especially in your back where your thumbs are located, in the front where your fingertips are, and in the lowest part of your abdomen below your belt line just above your groin. If you find an area that is not pushing out or tightening up very well, these are the areas that you need to work on. You can make this an exercise by placing your hands in your weakest areas and pushing out and tightening up. Hold for a second, release, and repeat 10-20 times or until fatigue. You can do this multiple times a day, every day. It is important to practice this in all position…lying on your back, stomach, each side, sitting, and standing.
As a side note, you should also be able to breathe into your abdomen (diaphragmatic breathing) at the same time you have created IAP. Here’s the test: Create IAP by pushing out and tightening up no more half way (less than 50% effort). Now breathe into your abdomen while you keep the pressure constant, especially on the exhale. This is very difficult for most people to do and is a further predisposing risk factor for back pain. The breathing component is beyond the scope of this article. I have written another article on this if you want to check it out…
If you practice creating IAP enough, you should be able to feel the pressure and tightening without your hands around your waist. Now it is time to use IAP when you move. For this new pattern to get automatically programmed into your nervous system, you need to consciously think about creating IAP right before every movement you make. And not only creating it, but MAINTAINING IT THROUGHOUT THE ENTIRE MOVEMENT!
These are the most important times you want to do this:
Any time you have to bend or lean forward, such as getting in and out of a chair or your car, leaning forward to pick something up from a table or the floor (whether it is light or heavy), getting things in and out of the refrigerator, lifting up your legs to put on pants, socks, or shoes, during strength/weight training exercises, etc. If you have to hold your breath when you do it, that’s okay.
The goal is to have the awareness to recognize when you remember to do this and when you don’t. There will be times when you catch yourself “in the act” and realize that you forgot to do it. This will happen in the beginning. The important thing is you recognized it and you will remember next time. If you make a habit of doing this long enough, it will become an automatic, subconscious activity like it once was before. Now, each time you move you will be protecting your spine and not injuring your spine.
Many people have trouble knowing for sure if they are creating IAP and maintaining it properly. The best professionals to consult if you need help with this is a chiropractor or physical therapist who is trained in Dynamic Neuromuscular Stabilization (DNS).
If fixing your bad back is a top priority, your best bet is to find a corrective (CBP) chiropractor who also uses DNS treatment and exercises.
Research has verified what I have talked about in this article…that improper alignment and lack of proper IAP regulation are predisposing causes of back pain. I hope this article has given you a better understanding why most of us eventually suffer from back pain and why it is such an epidemic problem in our society.
If you like this post, share it. Comment on it. Email me if you have questions about it. Thanks for reading…
Dr. Ryan Hamm
drhamm@drryanhamm.com

Dr. Ryan Hamm is a chiropractor in Arlington Heights and has been treating disorders of the spine and extremities for over 30 years. He specializes in posture and movement rehabilitation to resolve painful conditions of the musculoskeletal system. Dr. Hamm has been studying the most critical components people need for ideal posture and movement to minimize joint wear and tear. He has an Advanced Certification in Chiropractic Biophysics (CBP) Technique, a Dynamic Neuromuscular Stabilization (DNS) certified practitioner and a certified DNS Exercise Trainer.
References
Troyanovich SJ, Harrison DD, Harrison DE. Low back pain and the lumbar intervertebral disc: Clinical considerations for the doctor of chiropractic. J Manipulative Physiol Ther 1999; 22(2): 96-104.
Troyanovich SJ, Harrison DE, Harrison DD. Review of the Scientific Literature Relevant to Structural Rehabilitation of the Spine and Posture: Rationale for Treatment Beyond the Resolution of Symptoms. J Manipulative Physiol Ther 1998;21(1):37-50.
Harrison DE, Colloca CJ, Keller TS, Harrison DD, Janik TJ. Anterior thoracic posture increases thoracolumbar disc loading. Eur Spine J 2005:14:234-242.
Harrison DE, Cailliet R, Harrison DD, Troyanovich SJ, Harrison SO. A Review of Biomechanics of the Central Nervous System. PART I: Spinal Canal Deformations Due to Changes in Posture. J Manipulative Physiol Ther 1999; 22(4):227-234.
Harrison DE, Cailliet R, Harrison DD, Troyanovich SJ, Harrison SO. A Review of Biomechanics of the Central Nervous System. PART II: Strains in the Spinal Cord from Postural Loads. J Manipulative Physiol Ther 1999; 22(5):322-332.
Harrison DE, Cailliet R, Harrison DD, Troyanovich SJ, Harrison SO. A Review of Biomechanics of the Central Nervous System. PART III: Spinal Cord Stresses from Postural Loads and Their Neurologic Effects. J Manipulative Physiol Ther 1999; 22(6):399-410.
Harrison DE, Betz J, Ferrantelli JF. Sagittal spinal curves and health. JVSR 2009 July 31, pp 1-8.
Keller TS, Colloca CJ, Harrison DE, Harrison DD, Janik TJ. Influence of spine morphology on intervertebral disc loads and stresses in asymptomatic adults: Implications for the Ideal Spine. Spine Journal 2005; 5:297-305.
Harrison DD, Harrison DE, Janik TJ, Cailliet R, Haas JW, Ferrantelli J, Holland B. Modeling of the Sagittal Cervical Spine as a Method to Discriminate Hypo-Lordosis: Results of Elliptical and Circular Modeling in 72 Asymptomatic Subjects, 52 Acute Neck Pain Subjects, and 70 Chronic Neck Pain Subjects. Spine 2004; 29:2485-2492.
Harrison DD, Cailliet R, Janik TJ, Troyanovich SJ, Harrison DE, Holland B. Elliptical Modeling of the Sagittal Lumbar Lordosis and Segmental Rotation Angles as a Method to Discriminate Between Normal and Low Back Pain Subjects. J Spinal Disord 1998; 11(5): 430-439.
Kolar P, Sulc J, Kyncl M, Sanda J, Cakrt O, Andel R, Kumagai K, Kobesova A. Postural Function of the Diaphragm in Persons With and Without Chronic Low Back Pain. , J Orthop Sports Phys Ther, 2012;42:352-362,
Hodges PW, Cresswell AG, Daggfeldt K, Thorstensson A. In vivo measurement of the effect of intra-abdominal pressure on the human spine. J Biomech. 2001;34:347-353.
Hodges PW, Cresswell AG, Daggfeldt K, Thorstensson A. Three dimensional preparatory trunk motion precedes asymmetrical upper limb movement. Gait Posture. 2000;11:92-101.
Hodges PW, Eriksson AE, Shirley D, Gande-via SC. Intra-abdominal pressure increases stiffness of the lumbar spine. J Biomech. 2005;38:1873-1880. https://dx.doi.org/10.1016/j. jbiomech.2004.08.016
Hodges PW, Gandevia SC. Activation of the human diaphragm during a repetitive postural task. J Physiol. 2000;522 pt 1:165-175.
Hodges PW, Gandevia SC. Changes in intra-abdominal pressure during postural and respiratory activation of the human diaphragm. J Appl Physiol. 2000;89:967-976.
Hodges PW, Richardson CA. Altered trunk muscle recruitment in people with low back pain with upper limb movement at different speeds. Arch Phys Med Rehabil. 1999;80:1005-1012.
Kolar P, Sulc J, Kyncl M, et al. Stabilizing function of the diaphragm: dynamic MRI and synchronized spirometric assessment. J Appl Physiol. 2010;109:1064-1071. https://dx.doi. org/10.1152/japplphysiol.01216.2009


